Anyone following the coronavirus stuff closely enough to comment on things like
how worried should I be about delta variant?
do the vaccines still work against new variants? Will they keep working? Will they make new vaccines against the new variants, and how long will that take?
if I relaxed precautions after being fully vaccinated for two weeks, should I go back to extreme caution? Is traveling dumb right now?
BTW I think there was a strong message from govt that if you got the vaccine things could be more normal again, but now that seems to not be the case, and people are getting very mad about it.
The vaccines still work against Delta - I believe they are a bit less effective against symptomatic infection, but still very effective against actual hospitalization & death.
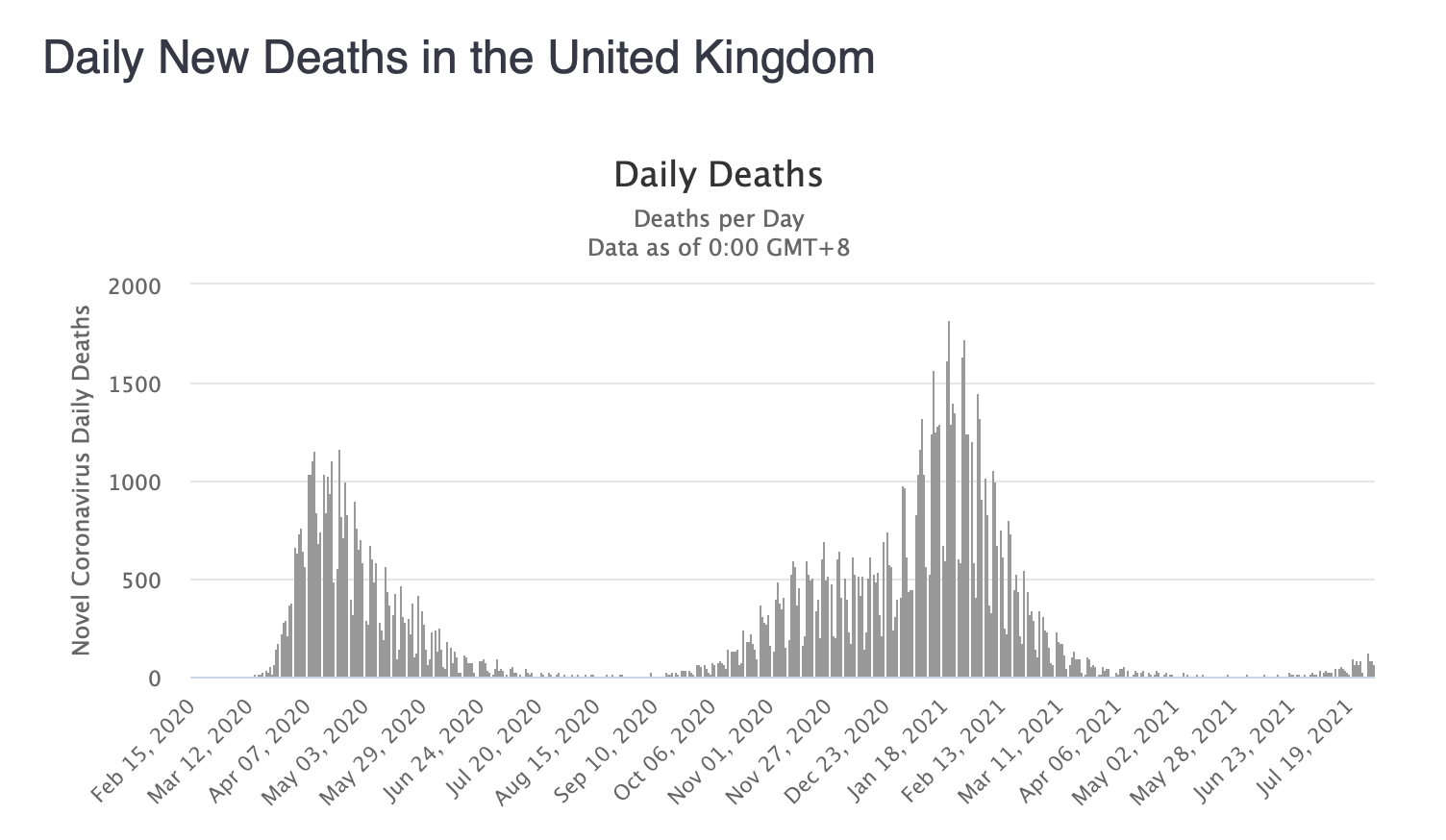
The numbers from UK are interesting - their population is highly vaccinated, and they saw a huge decrease in COVID cases once vaccinations started, but then a large increase again when the Delta variant started spreading:
The Delta variant is already spreading in the US, and is apparently the dominant variant. According to the numbers I have read, almost all (like, 99%+) COVID deaths in the US are among the unvaccinated. And of the deaths among vaccinated people, most of those were among people with major pre-existing conditions and ages 60+.
So if you are younger and otherwise healthy, then I don’t think you personally need to be very concerned about dying from COVID.
But on a society-wide level, I think continuing precautions like staying home if sick, proper hand-washing or sanitizing (that one should be a forever thing), and wearing masks inside should all continue to be practiced. I don’t think they should have ever stopped recommending that vaccinated people wear masks. You are unlikely to die from COVID, but vaccinated people can still get it, and I don’t think there’s any good evidence that they don’t spread it, so it makes sense to be cautious about that. (At this point in the US, I think it would make sense to strongly recommend masks for everyone, and for most people to be wearing them, but not to force everyone to wear them. Masks aren’t very invasive for most people.)
Besides vax helping reduce severity even when you get delta, UK deaths are also probably down due to the hospitals not being overwhelmed anymore (which is b/c of the vax helping, but the result is if you’re one of the ppl who does need hospital help, you can get better care atm since the system is less stressed).
The vaccines do seem to work against the new variants. We might need booster shots (Pfizer is already saying something about wanting them). That shouldn’t take long, since it would just be using the same vaccine again.
The team also estimated that beneficial mutations in the spike proteins of OC43 and 229E appear roughly once every two to three years, about half to one-third of the rate seen in the flu virus strain, H3N2.
(OC43 and 229E are both strains of coronavirus that cause the common cold in humans. They are not the only source of the common cold though. Flu viruses have mutations yearly, which is why we have yearly flu shots.)
So maybe the COVID-19 virus will turn into something like a flu or common cold, circulating regularly, and mutating enough that we need regular vaccines like we have with the flu shot. They could act like the other circulating coronaviruses, and mutate less often than the flu, which would mean we would only need covid shots every 2-3 years, instead of yearly like the flu.
As to how long vaccine development would take, I’m not really sure - the actual vaccine development itself was really really fast. The thing that took so long was the testing phases required by the governments. I don’t actually know how they do testing for the yearly flu vaccine, but they manage to get that out every year by October, so presumably they could do something similar with covid in the future, if it became a seasonal issue.
It depends what precautions you mean, what you consider extreme, etc.
For many people, wearing masks is considered extreme. But I still think that should be the norm if you are indoors anywhere besides your own home, or perhaps the home of other fully vaccinated people that you have a small “bubble” with.
If you are not at increased risk (e.g., not old, no serious health conditions), then I don’t think you personally need to worry about dying from covid. I have read the death rate for vaccinated people is so low it is essentially 0.00%, so less than 1 in 10,000. I have also seen other numbers like 0.01%, which is 1 in 10,000. (And even if you are at higher risk, I think the death rate is still very low, but I don’t know how low - maybe it’s more similar to the flu death rate?)
Whether or not travelling is “dumb” depends on where you are travelling, why, etc. I don’t think all travel is dumb. A lot of people have been separated from their families now for over a year, and I think it is important for people to, e.g., see their grandkids, parents, etc.
The flu has a 0.01% death rate, and covid seems to be lower than that among fully vaccinated people, so I don’t think it makes sense to put your whole life on hold to avoid something with a lower death rate than the seasonal flu.
(I have said before - I do still think masks make sense, but that’s partly because not everyone is or can be vaccinated, we still don’t have all the information about the variants, and because I personally don’t think masks are actually very invasive. BUT I don’t think masks should be required of everyone, especially not in places where the vaccine is available to everyone who wants it.)
But there are plenty of countries that still have high covid rates and low vaccination rates. So if you are talking about tourism travel to one of those areas, I would avoid that. And also consider that if you are travelling anywhere, then if you are going through airports, staying in hotels, etc, some of the people you will be exposed to won’t be vaccinated, and will be coming from higher risk areas.
If you personally are healthy & vaccinated, you are probably safe, but if you are going to be coming home to a house with higher risk people in it, that could be problematic for them. You are unlikely to die from covid, but you could catch it on your trip and bring it back to your higher risk family members.
Oh, another thing to consider when you are thinking about safety is the vaccination rate in your area or state.
The US as a whole currently has 50% of the population fully vaccinated, and 58% with one shot, and the individual states vary a lot.
Canada is 58.8% fully vaccinated, 71.7% with one shot.
UK is 57% fully vaccinated, 70.2% with one shot.
Australia is 14.7% fully vaccinated, 32.6% with one shot.
(All those numbers are from typing “vaccine rate” and then the country name into Google, which gives you a chart. They get their data from Our World In Data.)
Even if you are not concerned about actually dying, you might still be concerned about still getting covid. It will be inconvenient: you may have to quarantine (you should quarantine as much as possible if you get covid, even if your jurisdiction doesn’t require it), it will interrupt your work or any travel plans, it will make you ineligible to enter a lot of different buildings or to do certain types of appointments. So even if you live alone, have no high risk family members to consider, are fully vaccinated & healthy, etc, you may still want to try to avoid getting covid.
So in that case, you should keep track of the vaccination rates & also the current covid rates in your area, and take precautions accordingly. If the vaccine rates are low, or the covid rates start to increase, you will want to be more careful.
Also it’s riskier to travel somewhere with poor medical care. There’s a higher risk of getting covid and needing some care than the risk of dying. Having to get care while traveling can be a big hassle or just not be available to you where you are or being lower quality (and you could e.g. die from an infection while in the hospital). Also make sure you have travel insurance that will actually work for where you want to go. Some insurances won’t cover trips to some places they consider unsafe.
On a related note, some people travel to poorer countries to get plastic surgery or dentistry cheaper. I haven’t researched the details but that sounds like a bad idea.
When I think about masks I actually think there are at least 4 different types that are good in different scenarios. I personally have all 4 types of mask. I think that’s kinda unusual, but doesn’t have to be as they’re all now pretty widely available:
Self-protective mask - An N95, KN95, or similar filtering respirator with an exhalation valve, which in rare circumstances isn’t considered compliant with mask requirements.
All-protective mask - An N95, KN95, or similar without an exhalation valve.
Other-protective mask - A surgical mask - worse in terms of protection than all-protective and most of the protection is outgoing, but extremely cheap, light, and easy to fit.
Compliance mask - Cloth mask or similar. Better than nothing and originally a valid stop-gap measure at the beginning of the pandemic when better masks weren’t widely available. However now I think these are mainly useful as a convenient way to comply with mask requirements.
I find discussion of mask recommendations / requirements that do not address the different types of masks to be mostly unhelpful, because I think what people could/should wear depends greatly on the circumstances. When the CDC recommends masks most people will think of cloth masks or surgical masks which are the least effective.
An all-protective N95/KN95 with no exhalation valve has the downside at least for me that I find them difficult to fit properly and uncomfortable to wear for very long.
Before getting vaccinated, if I had to go out and be indoors with others (rare) I’d always wear a self-protective mask. I have a respirator with a silicone face cup and a replaceable filter that’s a much easier / better fit and much more comfortable than a disposable N95/KN95. It has an exhalation valve. It was my “go-to” for most of the pandemic. Shortly after the pandemic started my whole household became very well isolated and I thought the biggest risk was letting something get past that. The risk I posed to others was, objectively, miniscule so I never worried about the exhalation valve. The cloth mask and surgical masks I had were just backups or carried for ex: outdoor activities where I didn’t expect to encounter anyone but was always prepared just in case.
Once I and the rest of my household got vaccinated (and waited for full immunity to kick in) I stopped using the self-protective respirator. We weren’t “special”, and by the time we could get vaccinated anyone could and we were some of the last in our extended family to be eligible. And the vaccines are free & widely available. So a few weeks after I was vaccinated I considered anyone in the US who could be vaccinated and wanted to be vaccinated had been vaccinated. But because I started going out again my risk of being a carrier and infecting others went way up.
Currently in medical type settings like seeing the doctor or other settings where unvaccinated or immuno-compromised people might reasonably need to be, I’ll wear an all- or other-protective mask with no exhalation valve.
Currently in indoor social settings I deem optional like restaurants, most stores that sell stuff you can get online, or gatherings/events, if a mask is requested or required I generally wear a compliance (cloth) mask. If it’s not requested or required, I wear no mask at all.
My reasoning is as follows: Bad things can always happen. Getting severe/deadly COVID post-vaccination is a noise floor level risk to me personally and all of my household. Meaning, it’s similar to the risk of getting injured or killed in an accident travelling to or from the event, or being a violent crime victim, or catching some other severe disease etc. Getting inconvenience level COVID post-vaccination is an above noise-floor risk but similar to colds & flu in terms of risk and impact. Any optional social activity should be evaluated in light of all of those risks, and always should have been. If something isn’t worth those risks to me, then it isn’t worth doing and I don’t do it. Wearing an actually-effective mask like an N95, KN95, or respirator substantially interferes with my enjoyment of such activities & if I thought that was necessary I just wouldn’t do the activities. That was my policy between the start of the pandemic and getting vaccinated - I simply avoided optional indoor social activities.
The recent change in CDC guidelines does not affect my personal mask policies at all. It does affect the places that request or require a mask, which means I’m wearing my cloth mask a little more but my personal policy hasn’t changed.
During cold & flu season, or if COVID transmission rises to similar levels as last winter (which it easily might) I might choose to start protecting myself again with a self-protective mask and/or curtailing optional social activities.
Regarding others, there are 2 vaccination states (vaccinated or not) but 3 moral states (vaccinated, can’t be vaccinated[1], and chose not to be vaccinated). This is substantially different from the state of the world before vaccines were available at all or were available to everyone that wants one.
The vaccinated don’t need my protection. If they disagree, they can wear a self-protective mask. Which is what I will start doing again if I start seeing evidence that vaccine protection is waning either due to time or variants.
Those who can’t be vaccinated have my sympathy and do need to be protected in social settings they can’t reasonably avoid, which is why I wear an all-protective or other-protective mask in such settings. But those people should not be in optional social settings, especially without an all-protective or self-protective mask. If they are, then they’re voluntarily taking on an unnecessary and unreasonable risk and are they are no longer my responsibility to protect. What about people who can’t be vaccinated and are workers in optional social settings (like waiters in restaurants)? In my view if you have a medical condition that makes a particular type of job extra risky for you, you should get a different job. Maybe not tomorrow, but over time. This is a bit harsh, but it’s been true long before COVID. If you’re immuno-compromised or can’t be vaccinated against ex: measles then I think you shouldn’t be a waiter either. The pandemic has been around for a year and a half now, there’s been all kinds of government assistance and its reasonable to expect people for whom ex: waiter jobs are especially risky to have transitioned to something else.
Those who chose not to be vaccinated are not deserving of me going out of my way to protect them in optional social settings either. The vaccine refusers also, nearly 100% in my experience, refuse to wear any kind of mask themselves unless forced. They strongly resisted masks before the vaccines, and continued to socialize all through the pandemic. They’re dumb, and far too numerous, but frankly not my problem.
[1] “can’t be vaccinated” includes people with medical conditions that prevent them getting the vaccine or make getting the vaccine more risky than not. It also includes people with immuno-compromising conditions who got the vaccine but for whom vaccine effectiveness should reasonably be expected to be substantially less than normal.
I have my first vaccine scheduled for Monday. I had some doubts initially of potential long-term effects, but I learnt that all vaccines in history have had no long-term issues and if we see any negative effects they’re almost always in the first 90 days or so after being vaccinated.
I’ve also read some stories on reddit of people contracting COVID-19 even after being vaccinated, like one workplace that had 95%+ people vaccinated but has 20+ cases and counting, and another example of a wedding where vaccinated people contracted the virus. It definitely does reduce the severity of symptoms but I was considering attending some events after being vaccinated which I will no longer be doing. I’ll continue to stay at home and have groceries delivered etc.
Yeah, I agree. Ultimately the risks of the vaccine seem much lower to me than the risks of COVID-19 complications and issues, especially long-term stuff like lung damage.
If you look at the history of vaccines you know that virtually all long-term adverse effects of a vaccine occur between 15 and 30 days after you get the dose, 45 days at the most. When you get a vaccine allowed by the Food and Drug Administration (FDA), such as with the emergency use authorization, you have to wait 60 days from the time half the people in the trials got their last dose and observe safety before it can be used on the public. If almost all of the long-term adverse effects occur within 45 days, you’ve gone beyond that if you wait 60 days, so the chances of there being long-term effects are vanishingly small.
I was wrong about the 90 days number. It’s 45 days. So no long-term testing of vaccines are really required, unless a new vaccine breaks the precedent of all historical vaccines somehow (which is possible, so still likely worth the testing that we do)
FWIW, I would not trust Fauci. I understand him to be a political figure (rather than primarily scientist or doctor) who did poorly in the past (re AIDS) but maneuvered to maintain power anyway.
I agree with this. I think if everyone in your household is vaccinated, and no one has any conditions that make the vaccine less effective for them or make them more at risk, then you don’t need to be worrying about catching covid and actually being hospitalized or dying from it. It is there as a risk, but the numbers seem similar to the chance of dying from the flu (for vaccinated people).
I disagree with this. I don’t think the inconvenience of covid is similar to the inconvenience of the cold or the flu. If you get covid, you should quarantine while you are sick. (Some places require this, and some don’t, but I think everyone should quarantine if they get covid.) Even if you don’t fully quarantine, you will not be allowed to do certain things (e.g., medical appointments, work if you don’t work from home, travel, etc).
During normal times, this hasn’t been an issue with colds or flus at all. Right now, if you get a cold or flu, you won’t have to quarantine, but you will have some issues - you won’t be able to do certain appointments, travel, etc with symptoms. And some places will ask you if you’ve symptoms in the last 14 days, and won’t allow you to make an appointment if the answer is yes. Other places will differentiate if you’ve had a negative covid test vs if you haven’t.
So I think right now, it would is much more inconvenient to get sick than it normally is. And it is more inconvenient to get covid than a cold or flu. But taking steps to protect yourself from covid will also protect you from colds & flus, so you don’t really have to differentiate.
If someone is averse to the possibility of a 10-14 day quarantine, they might still want to put effort into avoiding getting covid (or getting sick at all), even if they (and all their household members) have a very low risk of serious side effects.
Quarantining doesn’t seem like a big impact to me because of how my life is set up. I was mostly quarantining for a year before I was vaccinated. When I went out at all, which was rare, it was mostly for things that could also be done by another member of the household or delayed for 2 weeks without a big impact. This is almost certainly not true for many / most people, so your point is generally valid.
But also, I think I’m confused about the right symptom response protocol. I think being strictly scrupulous is unrealistic / overly burdensome, and ~no one (or ~no one who gets allergies and headaches) actually is. I also don’t know what the right answer is. And I don’t think most other people do either.
I commonly get allergic reactions where I’ll get some combination of a runny or stuffed nose, sore throat, cough, sneezing, or headache. Some reasons I guess this is allergies not a virus are that it happened before COVID and it continued to happen last year at about the same rate even when no one had left the house for a week, and when they did for the 3 weeks before it was only to collect mail from a PO box when the post office was closed and no one was there and they wore a self-protective mask, everything coming in to the house was no-contact delivered and then wiped down with bleach rag or baked in the oven, etc. IOW, no plausible viral vector for it, and it happened repeatedly. It also isn’t constant (symptoms come and go). It also sometimes feels different from a cold/flu coming on even though they’re nominally the same symptoms, but the main way I find out is if I take an allergy med at bed time and it doesn’t get better at least while the med is in effect, it’s probably a virus instead of allergies.
Also sometimes I just get headaches - not severe / migraine type stuff but noticable enough to say “I have a headache”. Maybe allergies but maybe other causes like tension or caffeine withdrawal too. These never develop into anything else and I’d guess they’re highly unlikely to be any kind of virus.
My best guess, with pretty high confidence, is the last time I had any kind of virus was October 2019. It was either a cold or flu, similar to cold/flus I’ve had before. I can’t tell whether it was cold or flu because I had a flu vaccine so it could’ve been flu that the vaccine helped some with, or it could have just been a cold. Unpleasant, but didn’t knock me flat or anything. I had been travelling by air (so known high-risk exposure), I had primary symptoms for like a week and follow-on symptoms (mostly dry cough) for 2-3 weeks after that. Allergies and headaches don’t behave like that.
Point being, I am pretty confident I can tell after ~a day or so when I have a virus vs. having nominally similar symptoms that aren’t viral. Perhaps that confidence is misplaced.
If I had a headache (COVID symptom) but nothing else and my best guess is it wasn’t a virus, should I answer yes to COVID-related symptom questions anyway? Should I get a COVID test every time I have such symptoms? I’d guess that’d be about a test a month which seems really impractical and dumb. What about combination symptoms like runny nose and cough I attribute to allergies with high confidence? I dunno. Should my answer be different if I’d been consistently masking in public indoors vs. if I haven’t? Probably not. But if it should be different, should my answer also be different if I’d been wearing a highly protective respirator like an N95 vs. if I’d been wearing only a cloth mask? I’d guess yes. Cloth masks are better than nothing but significantly less protection than a real respirator.
I haven’t been in a position where I’ve been asked about COVID symptoms when symptoms I attributed to allergy / headache were recent. That’s a combination of luck and not doing much where I get asked such questions.
And is there any difference if I’m explicitly asked (which I was before getting vaccinated) vs. if there’s just some generic sign like “don’t enter if you’ve had COVID-like symptoms in the last 14 days”. The sign seems way more ignorable to me than the questions, but perhaps that’s wrong.
I would definitely answer yes to symptom questions / not enter buildings with signs if I had a suspicion the symptoms might be viral. But that’d be true whether the virus was a cold, flu, or COVID. In that sense, the inconvenience of having any virus has gone up, not COVID specifically.
And I am also unclear on what I should do beyond answering yes if I get symptoms that seem to me to be viral. Should I get a COVID test? Unless the symptoms are severe, I had a known exposure to COVID, or I’d recently had traceable non-household contacts I still don’t think I’d wanna get a test. Too many issues with false positives, false negatives, and delayed results when no decisions pertaining to my care or others’ exposure depend on the result. If I don’t get a COVID test should I quarantine like it was COVID? Dunno. Even with cold/flu before COVID I tended to mostly isolate, probably better than the average person trying to “quarantine”. The main exception before COVID was air travel - if I caught something on a flight out and knew I had it during a trip I’d still finish out the trip until I was home, mainly cuz of committed meetings and non-refundable high change-fee air tickets. Culture / logistics / finances / employer policies just didn’t support halting everything in a remote city for a week cuz you got a cold or mild flu. I haven’t flown since COVID but my guess is that’s changed.
If I did get a COVID test and it came back positive, sure I’d quarantine. I just think there’s a whole lot of pretty important unknowns before I’d ever get to that point.
Anyway, like I said I think I’m confused about the right approach and as a result perhaps I underestimate the impact of inconvenience-level COVID if I actually handled it right.
I realized as written this is a non-sequitur. What I had in mind was more like:
I think I’m confused about the right approach and as a result perhaps I underestimate the impact of not taking precautions against inconvenience-level COVID and then responding correctly to symptoms.